
Foot, Leg and Heel Pain
Abbots Langley Clinic offers comprehensive treatment for the entire body.
We often find that patients may experience pain and discomfort in areas of their body that are connected to other regions, even if those areas don’t seem to be the problem.
Our team of specialist consultants is highly qualified to examine and diagnose specific conditions thoroughly, many of which originate in the lower limbs and feet.
Below is information about the most common conditions we diagnose and treat:
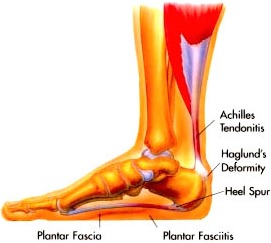
The two most common causes of pain in the bottom of the heel, the arch, or both the heel and the arch, are plantar fasciitis and heel spurs.
Plantar Fasciitis is an inflammation of the plantar fascia, which is a thick band on the bottom of the foot that is connected to the heel and extends forward to the ball of the foot. The inflammation usually occurs where the band attaches to the heel, but it can occur anywhere on the plantar fascia, causing pain.
A Heel Spur is a calcium or bone growth that protrudes from the bottom of the heel bone, within the fibers of the plantar fascia. When walking, the spur can cause micro-tears in the plantar fascia, leading to inflammation and pain in the heel, which may also affect the arch.
The main symptom of these problems is pain in the bottom of the heel or arch when first standing, which may improve with walking but return after continued walking, and subside after rest.
Causes of these conditions can vary and may be due to excessive pronation. Treatment for these conditions requires specialised knowledge and care.
Achilles tendinitis is an inflammation of the Achilles tendon, which connects the calf muscles to the heel.
This long and thick tendon allows us to move our foot downward, pointing the toes to the ground (plantarflexion).
The most common site of Achilles tendinitis is at the heel and up to 4 inches above it.
Most Achilles symptoms are caused by excessive pronation, which puts constant strain on the tendon.
 When children experience recurring heel pain, it is usually due to Sever’s Disease, whereas adults typically experience heel pain due to heel spurs or plantar fasciitis.
When children experience recurring heel pain, it is usually due to Sever’s Disease, whereas adults typically experience heel pain due to heel spurs or plantar fasciitis.
- Apophysitis is an inflammation of a growth plate.
- Calcaneus is the anatomical name of the heel bone.
- Sever’s Disease is an inflammation of the growth plate located at the back of the heel.
Sever’s Disease is most commonly seen in physically active girls and boys between the ages of 8 and 15. During these years, the growth plate is still “open” and has not fused into mature bone, making it more vulnerable to overuse injuries, often caused by sports activities.

Shin splints typically refer to pain in the front of the leg, anywhere between the ankle and the knee, or pain on the inner side of the lower leg. This pain is usually triggered by walking, running, or jumping and can even occur when standing still in extreme cases. If left untreated, the pain can become sharp and intense during weight-bearing activities, and may feel as though the muscle is being pulled off the bone.
Anterior shin splints usually involve the Tibialis Anterior Muscle, located in the front of the leg. This muscle, which attaches to the foot and flexes it upward toward the shin, is encased in a thin sheath. When the foot is pronated (rolling outward at the ankle, causing you to walk more on its inner aspect), the muscle can twist within its sheath, leading to tiny tears or inflammation and pain.
Posterior shin splints typically affect the Soleus and Tibialis Posterior muscles, which are located at the back of the knee and run down the back and inner side of the leg before attaching to the foot. Just like with anterior shin splints, when the foot is pronated, these muscles can become twisted, leading to tears, inflammation, and pain.
 One of the most common causes of knee pain in runners is due to “Runner’s Knee” or Patellofemoral Pain Syndrome. The symptoms of this condition may include:
One of the most common causes of knee pain in runners is due to “Runner’s Knee” or Patellofemoral Pain Syndrome. The symptoms of this condition may include:
- Pain near the kneecap (patella) and below it. The pain is located on the front of the knee, not deep within the knee joint.
- Sensation and sound of “grinding” when flexing and extending the knee.
- Pain after sitting with bent knees for a while, then standing up and walking.
- Knee pain while walking or running downhill, or walking down stairs.
- Pain when direct pressure is applied to the kneecap.
- Swelling around the patella when pain is present.

The patellar tendon connects the kneecap (patella) to the shin bone or tibia. This tendon is very strong and enables the quadriceps muscle group to straighten the leg.
The quadriceps actively straighten the knee during jumping to propel the individual off the ground and also help stabilise their landing. Thus, this tendon is subjected to significant stress, especially in individuals who regularly engage in sports involving jumping movements and sudden changes in direction.
With repetitive strain, the tendon may experience micro-tears and collagen degeneration, leading to a condition known as patellar tendinopathy or Jumper’s Knee. It’s important to differentiate this from patellar tendonitis, as the former involves tendon degeneration rather than inflammation.

Osgood-Schlatter disease is a common cause of knee pain in children and young athletes, typically affecting those between the ages of 10 and 16. It occurs due to rapid growth combined with high levels of physical activity, such as kicking, running, or jumping, which put intense strain on the quadriceps muscles. This strain leads to pain and swelling just below the knee. This condition primarily affects young teenagers, especially boys, and is rare in individuals over the age of 16.
The main symptom is pain just below the kneecap (patella), which can vary in severity and tends to worsen during and immediately after physical activity but eases with rest. The pain usually lasts for a few months, but in some cases can persist until the individual has finished growing, which can take up to two years.
A small, tender, bony bump may develop a few centimeters below the kneecap where the patellar tendon attaches to the tibia (shin bone). This bump is permanent but becomes painless over time.
Importantly, Osgood-Schlatter disease does not affect the actual knee joint, meaning knee movements remain normal. While symptoms typically occur under one kneecap, in up to one in three cases, it can affect the area under both kneecaps.

The key structures in the balls of the feet are the five metatarsal heads (the ends of the metatarsal bones that connect to the toes) and the protective fatty pad that cushions the ball of the foot.
With each step we take, we push off with our toes and the ball of the foot, propelling ourselves forward. This means that 100% of our body weight is exerted on these structures. Misalignment or inadequate fatty padding can cause pain in the ball of the foot.
Pain in this area can be caused by dropped metatarsal heads, Morton’s neuromas, fractures of the metatarsal bones, or excessive pressure from a high-arched foot.
 Calluses are areas of hard, dead skin found on the bottom of the feet, with the most common ones found on the balls of the feet.
Calluses are areas of hard, dead skin found on the bottom of the feet, with the most common ones found on the balls of the feet.
These areas of hard, dead skin can be diffuse and spread over a broad area, or they can be localised to a small area and be very deep, both of which can be very painful.
Calluses are a symptom of an underlying problem in the ball of the foot. A normal foot can comfortably carry weight without developing calluses and pain. When a callus occurs, it signifies a change in our metatarsals.
When one or more metatarsals bear more weight than they should, the skin under these bones becomes thick, hard, and painful.

The medical terms used to describe a bunion are Hallux Abducto Valgus and Hallux Valgus. A bunion is a complex deformity that results in:
- A bump that develops on the inner side of the foot, in the area where the big toe and the bone it connects to (called the first metatarsal) meet.
- The turning inward of the big toe, so that it presses against the second toe (the big toe is no longer straight).
Bunions are a progressive deformity, and if left untreated the bump will become larger, and the big toe will eventually lie over or under the second toe.
Orthotics can address many of the mechanical causes of a bunion. While orthotics do not actually correct a bunion deformity, if properly designed and made they can slow the progression of bunions. They are also made to redistribute weight away from pain in the foot that often accompanies bunion development.
In order for a bunion to form, the ligaments and tendons that hold the bones and joints together must be more flexible than normal. This abnormal flexibility is usually the result of a biomechanical foot defect called pronation, which disrupts the normal relationship between the big toe and the first metatarsal.
Pronation is a turning outward of the foot at the ankle, so that one has a tendency to walk on the inner border of the foot. When this occurs, we walk with an abnormal amount of our weight being forced on the big toe and first metatarsal, resulting in a bump on the inner side of the foot, and a big toe that is pushed toward the second toe.
When flat feet occur along with pronation, the foot becomes even more flexible and susceptible to bunion formation. Bunion progression may be accelerated by:
- Wearing high heels or pointed toe shoes
- Injury to the big toe, which may damage the first metatarso-phalangeal joint and speed up bunion formation.
- Arthritis of the first metatarso-phalangeal joint may cause the joint to become enlarged, leading to bunion formation.
- Some neurological diseases cause contractures of the joints of the feet and toes, helping bunions to form.
 Stress fractures are cracks in the metatarsal bones that typically occur without a significant injury to the bone.
Stress fractures are cracks in the metatarsal bones that typically occur without a significant injury to the bone.
They are usually brought on by excessive pressure applied to the bone, either suddenly or over time. These fractures are thin cracks in the metatarsal bone without separation of the fractured pieces.
It’s important to note that these fractures may not appear on an x-ray until the healing process begins, which can be up to 3 weeks after the injury.
 Morton’s Neuroma is a benign soft tissue mass that forms on the nerve which runs between the metatarsals in the ball of the foot.
Morton’s Neuroma is a benign soft tissue mass that forms on the nerve which runs between the metatarsals in the ball of the foot.
When two metatarsal bones rub together, they can pinch the nerve that runs between them. This repeated pinching or injury to the nerve causes it to swell, eventually leading to the formation of a benign mass at the site of the repeated injury.
This mass is known as Morton’s Neuroma, named after the physician who first described it in 1876.

The foot’s arch is responsible for absorbing shock and supporting our entire body. Every time we take a step, we put up to four times our body weight on our foot, depending on whether we are walking, running, or jumping.
Without the arch to absorb shock, the force of each step would eventually cause fractures or dislocations in the bones of the foot, leg, and lower back.
If left untreated, this could lead to a completely collapsed foot, which would no longer be able to absorb shock, resulting in constant pain in the foot and eventually affecting the knee, hip, and lower back.

Pronation refers to the outward turning of the foot at the ankle, causing a tendency to walk on the inner border of the foot. Over-pronation occurs when the foot and ankle pronate to a great degree.
You can test for pronation by observing the leg and foot from the back. If left untreated, pronation can lead to various issues such as heel spurs, plantar fasciitis, frequent ankle sprains, shin splints, weak and painful arches, and eventually knee, hip, and lower back pain.
TREATMENT OF PRONATION
CHILDREN
If pronation is diagnosed before the age of five, it can usually be treated in a way that aligns the bones and joints properly as the child continues to grow. This prevents the arch from collapsing and allows the leg muscles to enter the foot without twisting.
With proper and early treatment, the foot will not turn out at the ankle, and the child’s walking pattern will improve. Treatment for pronation in children may include: night braces, custom-made orthotics, and exercises.
These treatments are typically continued until the child’s growth is complete. In adulthood, custom-made orthotics may be necessary to prevent the pronation from recurring, as the foot tends to return to its original form if preventive measures are not taken.
Often, pediatricians wait too long, hoping that the child will “outgrow” the problem. By the time they realise that the child’s feet will not improve, it is too late to change the foot. In such cases, custom-made orthotics are used to prevent the pronation from becoming worse.

ADULTS
The main reasons custom-made orthotics are effective for pronation are:
- Pronation forces most of our weight onto the inner border of our feet. Custom-made orthotics redistribute the weight so that the entire foot bears its normal share of weight with each step.
- The foot will strike the ground normally when the orthotics are used, preventing shin splints, ankle sprains, knee and hip pain, lower back pain, nerve entrapments, tendonitis, muscle aches, bunions, hammer toes, and calluses.
- Custom-made orthotics support not only the arch as a whole but also each bone and joint that forms the arch, providing the specific support needed for each foot. Using over-the-counter arch supports is not sufficient, as they do not provide the proper support to each specific structure of the arch and foot.
- Custom-made orthotics reduce the twisting of the leg muscles as they enter the foot, thereby reducing Achilles Tendonitis, shin splints, ankle, knee, hip, and lower back pain, and leg cramps, and allowing the leg muscles to work more efficiently.
- Custom-made orthotics absorb a considerable amount of shock, helping to protect our feet, ankles, knees, hips, and lower back when we walk or run.
Your Health is Our Priority
Early diagnosis of a condition always provides the optimum opportunity for a fast and effective recovery, while minimising the possibility of reoccurence or long-term problems.
If you are suffering pain or discomfort, please call Abbots Langley Clinic on 01923 268787 to discuss your issue with a compassionate member of our team who will be happy to provide you with information and book and appointment at your convenience.
Orthotics Menu


Edward Buckwald
B.Sc. (Hons), Ost
PRINCIPAL OSTEOPATH and ORTHOTIC SPECIALIST

Julian Banton
M.Sc., Ost
OSTEOPATH and ORTHOTIC SPECIALIST
I never notice when I have my orthotics in, but I always know when I haven’t….. my back and feet ache.
Call 01923 268787 to book an appointment
Clinic Information

Opening Hours
| Monday – Thursday: | 8:30 am – 6:00 pm |
| Friday: | 8:30 am – 5:30 pm |
| Saturday: | 8:30 am – 2:00 pm |